











 Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
1 Introduction
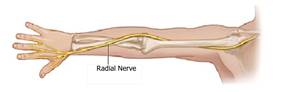
One of the five major branches of the brachial plexus is the radial nerve, it provides the arm and forearm with motor and sensory innervation (Lowe et al., 2002). Figure 1 sketches the nerve extension. Radial nerve palsy is one common injury to this nerve, symptoms can include pain, weakness, and loss of sensation along the back of the arm, forearm, and hand (Bumbasirevic et al., 2016). In general, paralysis hinders the mobility and extension of the wrist and fingers. Therefore, this disease is called “dropped hand” (Piña-Garza & James, 2019). After suffering a radial nerve injury, a person should always be subjected to arm rehabilitation to recover the mobility and operability (Niver & Ilyas, 2013).
Barton (1973) and Parry et al. (1981) highlight the importance of splinting to ease flexion of the fingers; there are a number of splinting solutions for the radial nerve palsy problem. The biggest challenge is to prevent over-stretching the denervated muscles and substitute the extensor muscle, effectively. Static splint stabilizes the wrist (Pearson, 1984) allowing the transmission of force to the flexors for power grip. Immobilization of the wrist only accentuates the inability of the fingers and thumb to open out of the palm (Colditz, 1987).
In the relevant literature there are several studies dealing with this problem. In Willand (2015), authors performs some experiments about daily muscle stimulation paradigm in rats, following nerve injury. Results show that re-innervation of muscle and functional behavioral metrics are enhanced with daily stimulation with the up-regulation of intramuscular neurotrophic factors as a potential mechanism. In Rodrigues et al. (2016), the evaluation of several subjects on carpal tunnel syndrome (𝐶𝑇𝑆) is carried out, to whom fulfill the criteria; a recovery method based on action potentials is applied. The response to electrical stimulation is faster than conventional methods.
In Ecuador, there are some investigations about rehabilitation, many of them for diverse sorts of injuries and different splint construction methods. In Universidad Católica Santiago de Guayaquil, was built a robotic hand controlled by the foot (Espinoza Morán, 2014). In the same way, students from Chimborazo proposed a prosthesis for the leg replacement (Romero Erazo, 2016), and posteriorly, it was presented a prototype by using a 3D printer (Andrade Holguín, 2016). Most of the investigations in 𝐸𝑐𝑢𝑎𝑑𝑜𝑟 are focused on the prosthesis construction but not in conjunction with the rehabilitation process. This work is one of the first about radial nerve palsy treatment.
In recent years, the rehabilitation process has been improved, however, there are some non-favorable issues related to rehabilitation; most centers require daily attendance and payment of the patient; for an extended period. On the one hand, some patients do not have the financial resources and mobilization that permits a successful rehabilitation process, and on the other hand, the technology of the public therapy centers limits the number of patients that can be treated at the same time (Vélez, 2017). Conventional methods are currently performed manually; that is, the physiotherapist performs manual movements to the patient’s wrist for some time according to the level of recovery.
This paper presents an autonomous rehabilitation system based on an electronic splint, capable of helping people who have suffered wrist and radial nerve injuries by mean of electric stimulation. The electronic splint is part of a system, assembled to collect information during the rehabilitation process, and storing into a database to be studied and analyzed by a physiotherapist, in order to make decisions about the routines that must be implemented in the splint, in terms of application time, operating frequency, current level, types of movements, and other configurable parameters.
The remainder of the paper is organized into four sections. Section 1 presents the introduction of the work. Section 2 describes the methodology; it is divided into two subsections; subsection 2.1 exposes the electronic devices and configurations, and subsection 2.2 explains the software used in the rehabilitation system. The evaluation and results are presented in section 3. Finally, section 4 concludes the paper.
2 Methodology
The rehabilitation system has been developed in Matlab, under an academic license. Matlab processes the data from sensors located in the electronic splint, trough a serial communication (RS232 protocol) and implements a database. The communication between the electronic splint and Matlab was done with the Arduino Uno board. In figure 2 is presented a general scheme of the rehabilitation system.

2.1 Electronic Splint Systems
The splint was designed using an arm immobilizer divided in two parts; one to support the forearm and other to move the hand. Considering the comfort of the patient, textile materials and surgical steel, were used. The two parts of the immobilizer were joined by servo motors, so that the wrist is free to be moved in the rehabilitation process. Figure 3 shows the initial prototype, and figure 4 shows the prototype under testing processes.


Electrical stimulation enhances nerve regeneration and helps in the functional recovery of the wrist and radial nerve injuries (Asensio-Pinilla et al., 2009), but it must be controlled and applied according to the patient recovery.
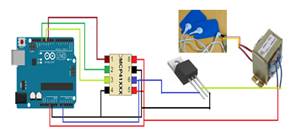
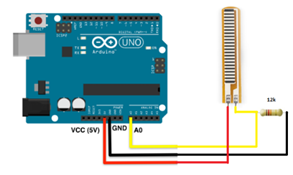
The electrostimulator consists of a flex sensor, a MPC41010 Single/Dual Digital Potentiometer (Microchip, 2003) and a servo-motor connected to the Arduino Uno board. The flex sensor controls the hand position, when the hand drops down, a signal is sent to the Arduino Uno to action the servo motor and restore the hand position. At the same time a 1:12 voltage transformer is used to have the signal current, through the electrodes, that is applied at the patient. To couple the current signal between the digital potentiometer and the voltage transformer, a NPN transistor has been placed. Figures 5 and figure 6, shows a general view of the setup.
The digital potentiometer MCP41010 controls the current intensity, in order to have safe levels. It needs one byte for control and one byte for data. Resistance can change from 180 to 255 Ω. The MCP41010 is connected to Arduino Uno board through the serial peripheral interface (SPI), pins 5 and 7 are connected to 5 𝑣 supply.
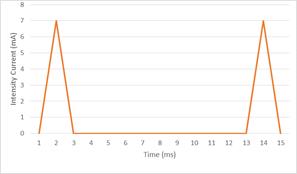
The relation of conversion of the voltage transformer is 1:12, connecting 3 𝑣 in the input it raises voltage up to approximately 40 𝑣. Now, if a 600 Ω resistor is connected, the intensity current should be equal to 60 𝑚𝐴. For the 83 𝐻𝑧 signal with a period of 12 𝑚𝑠; finally the high pulse is 7 𝑚𝐴, approximately.
The electric current signal, used for muscles stimulation, must be controlled in frequency, intensity and duration of impulses, accordingly to Pombo et al. (2004), to maintain the recommended levels for human rehabilitation. Low frequency relaxes the muscles and by contrast, high frequency contributes to the rehabilitation. To control the frequency, the duty cycle of the current intensity signal was changed. For 83 𝐻𝑧, the period of the signal was 12 𝑚𝑠, so, the time in high level was 1 𝑚𝑠 and the low level was 11 𝑚𝑠, according to equation 1. Figure 7 shows the 83 𝐻𝑧 signal with 𝑇=12 𝑚𝑠. Finally, by changing the high and low levels to 5 𝑚𝑠 and 50 𝑚𝑠, respectively, the signal of 18 𝐻𝑧 was generated. (1)
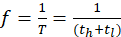
where:
The movements of the electronic splint were controlled by two servomotors of 20 𝐾𝑔, placed vertically on top of each other, as illustrated in figure 8, one servomotor controls up and down movement and the other right and left movement. Servomotors are commanded by a pulse-width modulation (PWM) signal from Matlab. Next section explains the software used for the system.

2.2 Software to control the rehabilitation system
The software for the rehabilitation system, previously shown in figure 2, implements some components, among them, graphical interface, database, and serial communications. The components were implemented by using Matlab, under an academic license. Arduino Uno libraries must be installed into Matlab, in order to control the board through a serial communication. Matlab sends commands to move servomotors according to the information received by the flex sensor. The installation of Arduino Uno libraries, was made from the Matlab interface, first clicking the Add-Ons icon, then choosing the “Get Hardware Support Package” option, and finally, selecting the Arduino Uno option.
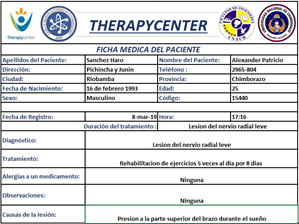
An important issue of the rehabilitation system is the database. The graphic user interface was also designed using Matlab, called TherapyCenter. The interface initially presents a form to capture data patients, for example, patient photography, personal information, injuries causes, diagnosis and treatment, allergies, and other medical observations about the injury. The software allows exportation, of the information, to an Excel spreadsheet where a code is assigned for each patient and the exact time and date of access to the rehabilitation system is recorded.
The program also provides three levels for selecting the severity of the injury, which are, minimal, normal, and severe. According to the selected injury level, the time of treatment fluctuates from one week, one month or six month of application, respectively. The system is accessed through credentials, for medical personnel and patients.
3 Results
In this sections are presented the results of the rehabilitation system, among them, the software results, the electronic splint under test, and the electrostimulator results.
3.1 Data base storing
Therapycenter allows inserting the information of the patient and exporting to an excel spreadsheet. Figures 9 and 10 depict the user interface and the exported file. The program automatically assigns a unique identification code for each patient, that is also used as password to access to the software. This guarantees access of authorized users to the information.

3.2 Electronic splint testing
The system was evaluated in the laboratories of the Physiotherapy department of National University of Chimborazo. It was then tested in a patient who initially had 10% of wrist mobility. The rehabilitation process consisted of five daily sessions with different duration for eight consecutive days. The progress was evaluated by mean of the daily variation of the movement angle of the wrist.
To establish a reference system that allows evaluating the progress in the rehabilitation, two perspectives are used. Figure 11(a) shows the system for hand movement from bottom to top. Whereas, figure 11(b) shows the reference system for the movement from left to right, both uses the normal position of the hand in 90 degrees.
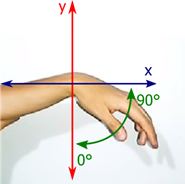
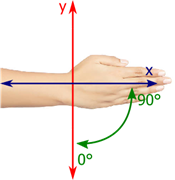
Once, the reference systems have been established, the electronic splint was tested for eight days. A person, who suffered a low level palsy, with 10% of hand mobility, used the rehabilitation system. According to figure 11(a), the position of the hand in ninety degrees represents the 100% of mobility, it means that a person with 10% of mobility, can only move the hand from 0 to 9 degrees.
Tables 1, table 2, and table 3 report the time, duration and the results of day one, four and eight, respectively, also the angles of application and the recovery progress, are reported. Angles are measured from the turn of the servo motor applied to raise up the hand. The recovery percentage is computed according to the degrees measured after the rehabilitation session, the patient, manages to raise up and move laterally the hand, by himself, until approaching the 90 degrees.
Table 1 : Data collected on the first day for 2 minutes.
| Time | Up-Down Angle(degree) | Left-Righ Angle(degree) | Progress(%) |
| 08:00 | 71.42 | 11.00 | 11.36 |
| 11:00 | 78.70 | 7.50 | 10.77 |
| 14:00 | 83.47 | 2.00 | 12.66 |
| 17:00 | 86.85 | 0.60 | 10.40 |
| 20:00 | 89.08 | 1.40 | 11.76 |
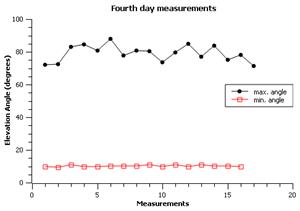
Table 2: Data collected on the fourth day for 1 minute.
| Time | Up-Down Angle(degree) | Left-Righ Angle(degree) | Progress(%) |
| 08:00 | 77.52 | 9.70 | 40.45 |
| 11:00 | 79.20 | 11.70 | 45.20 |
| 14:00 | 83.07 | 0 | 59.25 |
| 17:00 | 82.95 | -0.40 | 50.85 |
| 20:00 | 88.28 | -0.60 | 48.09 |
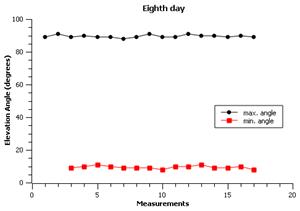
Table 3: Data collected on the eighth day for 15 seconds.
| Time | Up-Down Angle(degree) | Left-Righ Angle(degree) | Progress(%) |
| 08:00 | 75.05 | 12.80 | 95.52 |
| 11:00 | 75.55 | 12.10 | 94.36 |
| 14:00 | 82.92 | 3.20 | 96.21 |
| 7:00 | 87.23 | 4.70 | 98.21 |
| 20:00 | 89.07 | -3.80 | 99.12 |
First day, the five sessions were of 2 minutes, obtaining a rehabilitation progress of 11 % around. The fourth day, the progress was near of 50 %, the wrist can move 45 𝑜 . The eighth day, the movement of the hand was almost complete, and the progress was 96.68 %. The hand reached the 90 𝑜 of mobility and held horizontal position.
During the rehabilitation process, the data were collected in real time. Figure 12 shows the minimum and maximum angles of movement and elevation. The objective was to held the hand in horizontal position, when the rehabilitation process had been completed; it is presented in figure 13.
The data of the rehabilitation process was stored in the GUI of Matlab, after exported to an excel spreadsheet, that is a basic package of office software. The information allows the physiotherapist personnel to have full control of the process and statistic information in a format that could be easy to analyze, and export to other common formats.
3.3 Electrostimulator
The most important parameter that have to be controlled, is the current signal for the electrostimulator. The amplitude of the current was controlled varying the value of the resistance of the digital potentiometer. The electrostimulator is formed by the flex sensor, the electric system, electrodes and the communication with the computer. Sensor flex is located in the superior face of the wrist, as illustrated in figure 14(a), a flexion changes the resistance in the terminals of the sensor and an electrical signal is sent through the electrodes, placed on the forearm, as illustrated in figure 14(b).

[ (a) Flexsensor in the wrist]
[(b) Electrodes placement]

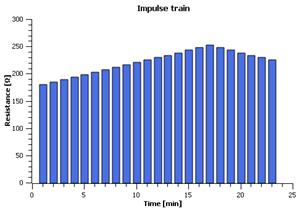
The electrostimulator operates in three different modes depending on the level of injury. Level one can operate without the electronic splint, while levels two and three operate along the splint. Level one is used for relaxing the muscle at 18 𝐻𝑧 frequency and for contracting the muscle with 83 𝐻𝑧. In this mode the flex sensor sends the signal to rise up the hand if it drops down. Level two and three act during the rehabilitation session helping muscles to contract and relax while the splint moves the hand. The difference between level two and three is the amplitude of the current signal. Level tree is used for strong injuries. Stimulation is a pulse train signal with amplitude and duration according to recommendations for neuromuscular recovering (Marqueste et al., 2004). Figure 15 illustrates the value of the control resistance for controlling the amplitude of the signal.
4 Discussion
Most of conventional methods for rehabilitation of the radial nerve are based on daily sessions assisted by a physiotherapist for relative long periods of time. Other options include orthopedic splint or surgery. The results of the conventional methods have shown to be successful, however they take a long time and could be expensive for the daily payment that frequently occurs.
Today the advancement and demand for technology is high, this encourages the use of telemedicine and biomedical systems. The rehabilitation system presented here, is an interesting option, which presents four advantages in comparison with conventional methods:
• The physical therapist personnel is not required all time,
• The system consist of a portable splint,
• The payment is not daily,
• The complete rehabilitation implies lower time.
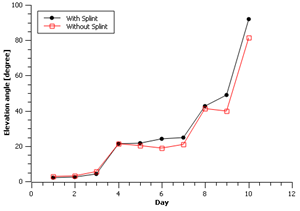
An advantage worth mentioning is that the recovery time is reduced. Although, it is not a significant difference, it has been possible to decrease the number of sessions in comparison to conventional methods. Figure 16 shows a comparison between the angle of mobility reached by a person using the proposed splint versus another with conventional methods.
A disadvantage of the system is ergonomics, since it has been designed for a single treatment. And the dimensions cannot be attached to anyone.
5 Conclusion
From the conducted study, it can be concluded that it is possible to build a rehabilitation system using low-cost electronic elements, with results comparable to traditional methods. A patient using the proposed system may have more stability on the hand than a person with conventional methods considering the similar duration of the rehabilitation.
Matlab programming software is an essential tool in the development of multi-platform systems, due to the compatibility and availability of libraries it was possible to carry out the Arduino-Matlab communication.
The rehabilitation system presented in this work allows the remote monitoring of the progress of the rehabilitation. The database stores the information of each patient and the results that are updated for each new session.

