










 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
The Earlobe crease (ELC) - Frank’s sign - is a wrinkle extending from the tragus to the outer border of the earlobe.(1) The documented association between ELC and coronary artery disease,(2) encouraged the search of other vascular correlates of this easily detectable skin sign. Some studies have linked ELC with peripheral artery disease, cerebrovascular events, and extracranial carotid atherosclerosis.(3)(4)(5) On the other hand, it has been suggested that ELC may be an age-related innocent bystander, and its value for predicting the occurrence of cerebrovascular events is still controversial.(6)
There are no studies addressing the potential association between ELC and intracranial atherosclerosis. During the conduct of the Atahualpa Project, one study participant with ELC was found to have severe (but asymptomatic) intracranial atherosclerotic disease.(7) This case - together with the lack of information in the literature - motivated the present population-based study, in which we aimed to assess the association between high calcium content in the carotid siphons (used as a surrogate of intracranial atherosclerosis) and ELC in community-dwelling adults living in Atahualpa (a rural Ecuadorian village).
METHODS
Study population
The population of Atahualpa is homogeneous regarding race/ethnicity, socioeconomic status, dietary habits and overall living conditions, as detailed elsewhere.(8) Almost all men belong to the blue-collar class and most women are homemakers. These consistencies reduce the risk of hidden confounders and make Atahualpa an optimal setting for the practice of epidemiological studies.
Study design
Atahualpa residents aged ≥40 years identified during annual door-to-door surveys who consented for the practice of a head CT and examination of the earlobes were enrolled. Women of child-bearing age underwent a pregnancy test before the study, and those who were positive were rescheduled for a CT after delivery. Using a population-based cross-sectional design, we assessed the association between high calcium content in the carotid siphons and ELC presence, after adjusting for age and other relevant confounders (see below). The I.R.B. of Hospital-Clínica Kennedy approved the study.
Earlobe examinations
Both earlobes were examined with the subject in the sitting position. An ELC was considered to be present when the individual has a wrinkle extending from the tragus to the outer border of the earlobe (Figure 1). Subjects with creases related to earrings and those who have physical damage distorting earlobe anatomy - precluding proper characterization of ELC - were excluded. Two investigators, blinded to each other’s assessments and to imaging data, assessed the earlobes. Inter-rater agreement was excellent (kappa=0.95), and discrepancies were resolved by consensus.

Neuroimaging protocol
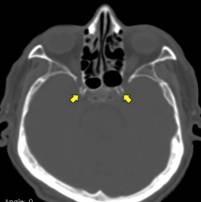
CTs were performed with a Philips Brilliance 64 CT scanner (Philips Medical Systems, The Netherlands). Slice thickness was 3mm, with no gap between slices. CT digital images were viewed on the Osirix Medical Imaging software (Pixmeo, Geneva, Switzerland) using the bone window setting to identify and grade carotid siphon calcifications. Using a previously proposed scoring method, individuals were stratified into those with low and high arterial calcium content.(9) Low calcium content was defined as the absence or near-absence of calcification, or as the presence of tiny scattered calcifications. High calcium content was defined as the presence of uni- or bilateral thin confluent, or thick - interrupted or continuous - calcifications (Figure 2). Two readers, blinded to ELC assessment, independently reviewed the studies (kappa=0.78) and resolved discrepancies by consensus.
Clinical covariates investigated
Demographics and cardiovascular risk factors were selected as confounding variables. Cardiovascular risk factors were assessed through interviews and procedures previously described in the Atahualpa Project, by the use of the American Heart Association criteria to assess smoking status, physical activity, diet, the body mass index, blood pressure, fasting glucose, and total cholesterol blood levels.(10)
Statistical analyses
Data analyses are carried out by using STATA version 15 (College Station, TX, USA). In univariate analyses, continuous variables were compared by linear models and categorical variables by x 2 or Fisher exact test as appropriate. Logistic regression models were fitted to evaluate the association between high calcium content in the carotid siphons (dependent variable) and ELC presence, after adjusting for the aforementioned confounders.
RESULTS
Figure 3 is a flow diagram depicting the process of enrollment and the reasons for not including potentially eligible individuals at each step of this process. From a total of 898 community-dwellers aged ≥40 years enrolled in the Atahualpa Project, 741 (83%) underwent a head CT. Of these, 46 had died or moved out the village between the practice of CT and the current study, and 44 were excluded because of earlobe deformities or creases related to earrings.

Figure 3 Flow diagram depicting the process of enrollment and the reasons for not including potentially eligible individuals at each step of this process.
The mean age of the 651 participants was 59.7±12.8 years and 350 (54%) were women. A body mass index ≥30 kg/m2 was noticed in 184 (28%) persons, blood pressure ≥140/90 mmHg in 200 (31%), fasting glucose ≥126 mg/dL in 159 (24%), and total cholesterol levels ≥240 mg/dL in 77 (12%). Twenty-seven (4%) participants were current smokers, 40 (6%) had a poor diet, and 52 (8%) had poor physical activity. ELC was present in 225 (35%) individuals. CT readings revealed low calcium content in the carotid siphons in 508 (78%) participants, and high calcium content in the remaining 143 (22%).
Characteristics of participants across categories of ELC and calcium content in the carotid siphons are detailed in Table 1. In univariate analyses, individuals with ELC were older (p<0.001) and more often men (p<0.001) than those without ELC. Some other covariables had borderline significance, including high blood pressure (p=0.064) and high fasting glucose (p=0.067) in persons with ELC than in those without. On the other hand, individuals with high calcium content in the carotid siphons were older (p<0.001), and had more often high blood pressure (p<0.001) and high fasting glucose (p<0.001) than those with low calcium content. In contrast, a body mass index ≥30 Kg/m2 showed a significant inverse relationship with the presence of high calcium content in the carotid siphons (p<0.001), which is explained by a mechanism of obesity paradox previously described in Atahualpa residents.(11)
Table 1 Characteristics of Atahualpa residents according to the presence of an earlobe crease and the severity of carotid siphon calcification (univariate analyses).
| Total series (n=651) | Earlobe crease | Calcium content in the Carotid Siphons | |||||
| Absent (n=426) | Present (n=225) | p value | Low (Grades 1-2) (n=508) | High (Grades 3-4) (n=143) | p value | ||
| Age, years (mean ± SD) | 59.7 ± 12.8 | 57.5 ± 12.6 | 64 ± 11.9 | <0.001 | 57.4 ± 12.1 | 68.1 ± 11.5 | <0.001 |
| Women, n (%) | 350 (54) | 247 (58) | 103 (46) | 0.004 | 283 (56) | 67 (47) | 0.075 |
| Current smokers, n (%) | 27 (4) | 17 (4) | 10 (4) | 0.417 | 23 (5) | 4 (3) | 0.479 |
| Poor physical activity, n (%) | 52 (8) | 40 (9) | 12 (5) | 0.096 | 36 (7) | 16 (11) | 0.154 |
| Poor diet, n (%) | 40 (6) | 29 (7) | 11 (5) | 0.424 | 30 (6) | 10 (7) | 0.777 |
| Body mass index ≥30 K/m2, n (%) | 184 (28) | 114 (27) | 70 (31) | 0.279 | 160 (31) | 24 (17) | <0.001 |
| Blood pressure ≥140/90 mmHg, n (%) | 200 (31) | 120 (28) | 80 (36) | 0.064 | 136 (27) | 64 (45) | <0.001 |
| Fasting glucose levels ≥126 mg/dL, n (%) | 159 (24) | 94 (22) | 65 (29) | 0.067 | 101 (20) | 58 (41) | <0.001 |
| Total cholesterol ≥240 mg/dL, n (%) | 77 (12) | 56 (13) | 21 (9) | 0.192 | 57 (11) | 20 (14) | 0.632 |
Univariate logistic regression showed a borderline (non-significant) association between high calcium content in the carotid siphons and ELC presence (OR: 1.44; 95% C.I.: 0.99 - 2.12; p=0.057), which disappeared when age was added to the model (OR: 0.98; 95% C.I.: 0.65 - 1.48; p=0.923). Then, a multivariate logistic regression model, adjusted for demographics and cardiovascular risk factors, also showed no association between high calcium content in the carotid siphons and ELC presence (OR: 0.97; 95% C.I.: 0.63 - 1.49; p=0.890). In this model, covariates remaining significant were age (p<0.001), sex (p=0.043), the body mass index (p=0.007), and high fasting glucose (p<0.001).
DISCUSSION
This study showed a borderline (non-significant) association between high calcium content in the carotid siphons and ELC presence in univariate analysis. This association totally disappeared when age and other covariables were added to regression models.
As noted, there are no studies attempting to assess the association between intracranial atherosclerosis and ELC. Therefore, our results cannot be compared with other series. On the premise that atherosclerosis is a systemic disease often affecting different vascular beds, we may interpret our findings on the light of other studies assessing the association between ELC and extracranial carotid artery atherosclerosis or peripheral artery disease.(3)(4)(12)(13)(14) Such studies have shown contradictory results. In one study ankle-brachial index (ABI) determinations were significantly lower (abnormal) in patients with ELC than in those without [4]. These results contrast with other studies showing no association between ELC and abnormal ABI determinations.(12) Regarding the relationship between extracranial carotid artery atherosclerosis and ELC presence, some studies have shown a significant association between both variables,(3)(13) while others did not.(14)
Most of the aforementioned studies have been flawed by either biased selection of participants, small sample sizes, or inadequate selection of statistical models according to the study design. This explains the inconsistent results. The present study followed a more rational methodology, including a population-based design with unbiased selection of participants, and selection of proper statistical models. These factors represent major strengths of our study. Potential limitations are the cross-sectional design and the fact that Atahualpa residents might not be representative of people from other ethnic groups.
Information on the pathogenic mechanisms explaining how ELC might correlate with atherosclerosis is limited. It has been suggested that abnormalities in collagen metabolism, involved in atherosclerosis progression, may also occur in the skin and are responsible for the presence of ELC in subjects with atherosclerosis.(15) In addition, it is possible that the ELC might be genetically determined and related to atherosclerosis, which might explain its different correlates according to race/ethnicity.(2) However, these hypothesis need to be confirmed.
In conclusion, the present study shows no association between intracranial atherosclerosis and ELC presence. In view of the paucity of information on this topic, further studies are needed to define whether the ELC could be considered a marker of intracranial atherosclerosis and a risk factor for cerebrovascular events.

