Case Report
All That Restricts Is Not Stroke: A Case Series Of Brain Imaging Findings In Infective Endocarditis.
Todo Lo Que Restringe No Es Enfermedad Cerebrovascular: Una Serie De Casos De Hallazgos De Imágenes Cerebrales En Endocarditis Infecciosa.
Cheruba Jonathan1
Senthil N1
Sowmya G1
Lakshmi-Narasimhan Ranganathan2
Ramesh Rithvik2
1Sri Ramachandra Institute of Higher Education and Research, Department of General Medicine. Porur, Chennai, India.
2Sri Ramachandra Institute of Higher Education and Research, Department of Neurology. Porur, Chennai, India. <rithvy@gmail.com>
Summary
Infective endocarditis is a systemic illness characterized by infection and inflammation of the endocardium which produces symptoms due to local causes and embolization. One of the sites of embolism is the central nervous system. Cerebral magnetic resonance imaging (MRI) exhibits greater sensitivity than computed tomography (CT) when detecting covert lesions like cerebral microbleeds and asymptomatic embolisms. There are specific patterns on cerebral MRI that prompt the diagnosis of infective endocarditis. This is a retrospective case series with the collection of data from 3 patients, who were encountered in the emergency and intensive care departments. All three patients had clinical features secondary to a shower of multiple emboli detected on MRI brain as multiple bi-hemispheric and multi-circulation foci of diffusion restriction. They were presumed initially to be cardioembolic in origin, which after targeted investigation were found to be due to infective emboli from IE. Bi-hemispheric scattered diffusion restricting foci can mislead the treating physician into evaluation for stroke secondary to cardioembolism including the hunt for an occult atrial fibrillation which can delay treatment required in IE. Distinguishing between septic and other cardioembolic lesions will result in the optimum management of such cases.
Keywords: Infective endocarditis; stroke; MRI in IE
Resumen
La endocarditis infecciosa es una enfermedad sistémica caracterizada por infección e inflamación del endocardio que produce síntomas por causas locales y embolización. Uno de los sitios de embolia es el sistema nervioso central. La resonancia magnética cerebral (MRI) exhibe una mayor sensibilidad que la tomografía computarizada (CT) cuando detecta lesiones encubiertas como microhemorragias cerebrales y embolias asintomáticas. Existen patrones específicos en la resonancia magnética cerebral que impulsan el diagnóstico de endocarditis infecciosa. Esta es una serie de casos retrospectiva con la recopilación de datos de 3 pacientes, que fueron atendidos en los departamentos de urgencias y cuidados intensivos. Los tres pacientes tenían características clínicas secundarias a una lluvia de múltiples émbolos detectados en la resonancia magnética del cerebro como múltiples focos de restricción de difusión bihemisféricos y de circulación múltiple. Inicialmente se supuso que tenían un origen cardioembólico, pero tras una investigación específica se determinó que se debían a embolias infecciosas por EI. Los focos bihemisféricos que restringen la difusión dispersa pueden inducir a error al médico tratante a realizar una evaluación de una enfermedad cerebrovascular secundaria a cardioembolismo, incluida la búsqueda de una fibrilación auricular oculta que puede retrasar el tratamiento requerido en la EI. La distinción entre lesiones sépticas y otras lesiones cardioembólicas dará como resultado el tratamiento óptimo de tales casos.
Palabras clave: Endocarditis infecciosa; ictus; resonancia magnética en Endocarditis Infecciosa
Introduction
Infective endocarditis (IE) is an infrequent yet severe ailment with a substantial propensity for fatality and affliction. There are various clinical presentations ranging from heart failure, pyrexia of unknown origin, and infarcts in end organs due to septic emboli. The fatality is high at 20% for both native and prosthetic valve endocarditis cases. Extracardiac symptoms are due to septic emboli which may be symptomatic or asymptomatic. Neurological symptoms may be varied such as headache, focal neurological deficits, seizures, altered sensorium, meningitis or transient ischemic attack which are all nonspecific. Brain imaging can reveal multiple bi-hemispheric infarcts which, in the setting of neurological symptoms can bias the treating physician toward the evaluation and treatment of ischemia. Herein we present a case series where findings on cerebral MRI along with the clinical presentation conversely prompted the diagnosis of IE.
Case series:
Case 1:
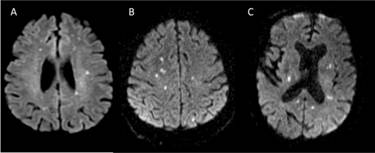
A 73-year-old male presented with sudden-onset right upper limb weakness and pedal oedema lasting for 5 days. He had a history of chronic kidney disease (CKD) on maintenance dialysis, diabetes mellitus, hypertension, coronary artery disease (CAD), and a prior left hemiparesis following an old cerebrovascular accident (CVA) with minimal residual deficit. An MRI of the brain revealed multiple small non-hemorrhagic diffusion-restricted areas in the bilateral cerebral hemispheres, gangliocapsular region, pons, and cerebellar hemisphere, suggesting an embolic stroke (Figure 1A). During his hospital stay, the patient experienced paroxysmal atrial fibrillation, which was managed with beta-blockers. Surprisingly, a 2D Echo revealed vegetation at the tip of the right atrioventricular valve, leading to empirical antibiotics and antiplatelet therapy. Blood cultures grew Enterococcus faecalis, and antibiotic treatment was adjusted. Subsequently, the patient deteriorated requiring inotropes and NIV. He also underwent intermittent slow low-efficiency dialysis (SLED). Due to financial constraints, the patient was transferred to another facility for further management.
Case 2:
A 73-year-old male, presented with reduced responsiveness for 1 day. He was status post mitral valve replacement, on anticoagulation. MRI brain done showed multiple areas of diffusion restriction bilateral cerebral hemispheres, basal ganglia and cerebellar hemispheres (Figure 1B). Transthoracic echocardiogram showed dilated left and right atria, prosthetic valve with no worsening regurgitation. Blood cultures sent for evaluation of altered sensorium subsequently grew Steptococcus agalactaciae and he was initiated on intravenous antibiotics. Transesophageal echo showed the presence of 12 x 9mm pedunculate mass attached to atrial aspect of mitral valve. Patient received 4 weeks of antibiotics during hospital stay and was planned to continue the same for 2 more weeks and remained symptomatically stable.
Case 3:
51-year-old male, retro positive status presented with fever and altered sensorium for the past 12 days. MRI brain was done which showed multiple punctate foci of diffusion restriction with corresponding T2Flair changes in bilateral frontal, parietal, left temporal, and bilateral cerebellar hemispheres (Figure 1C). Cerebrospinal fluid analysis additionally showed neutrophilic pleocytosis, elevated protein 84.9, with cultures and Gram stain showing no growth. He was initiated on intravenous antibiotics. Examination revealed splinter hemorrhages in his fingertips. 2D echo showed new regional wall motion abnormalities and EF 45 % with evidence of vegetation over the mitral valve. At the end of two weeks of antibiotic treatment, the patient was symptomatically better, and was lost to follow-up. (Figure 1)
DISCUSSION
Symptomatic cerebral ischemic or hemorrhagic events occur in about 30% of infective endocarditis (IE) patients, while asymptomatic events are detected in approximately 60% (1)(2) . MRI is more sensitive than CT for identifying covert lesions like cerebral microbleeds and embolisms (3) . However, routine cerebral imaging for IE diagnosis and management requires further validation. According to the American Heart Association's guidelines routine CNS imaging is not recommended for asymptomatic patients while in contrast, the European Society of Cardiology advocates for cerebral MRI in cases where IE diagnosis is uncertain but clinical suspicion is high, including asymptomatic patients (2)(4).
Neurological complications in IE can vary widely, and symptoms may be the primary indicators due to systemic septic embolization (1)(5). The CNS is the most common site of embolization (65%), mainly ischemic in nature. Other lesions include microbleeds, hemorrhagic lesions, brain abscesses, meningitis, and intracranial mycotic aneurysms. Ischemic lesions can vary in number, location, and diffusion restriction, making them appear similar to other thromboembolic causes (1).
IE-related lesions are often multiple in number, and various sizes, and can involve both hemispheres and all circulations simultaneously. Cortical lesions are common in both IE and other thromboembolic strokes, but IE lesions may be multiple and in distal cortical branch territories (6)(7).
Cerebral MRI in IE serves two purposes: identifying covert cerebrovascular complications in suspected IE cases and aiding in IE diagnosis in those with nonspecific neurological complaints. When ischemic and cerebral microbleeds coexist, it should raise suspicion for infective endocarditis (8)(9).
In conclusion, in the context of multiple foci of diffusion restriction in brain imaging, especially with an ambiguous clinical presentation IE has to be considered in one of the differentials. The judicial use of cerebral MRI will aid in the early detection of this condition and knowledge of distinguishing features of these lesions will help in timely management.
REFERENCES
Cantier M, Mazighi M, Klein I, et al. Neurologic Complications of Infective Endocarditis: Recent Findings. Curr Infect Dis Rep. 2017 Sep 19;19(11):41. https://doi.org/10.1007/s11908-017-0593-6
[ Links ]
Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015 Nov 21;36(44):3075-3128. https://doi.org/10.1093/eurheartj/ehv319
[ Links ]
Vitali P, Savoldi F, Segati F, et al. MRI versus CT in the detection of brain lesions in patients with infective endocarditis before or after cardiac surgery. Neuroradiology. 2022 May;64(5):905-913. https://doi.org/10.1007/s00234-021-02810-y
[ Links ]
Baddour LM, Wilson WR, Bayer AS, et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation. 2015 Oct 13;132(15):1435-86. https://doi.org/10.1161/cir.0000000000000296
[ Links ]
Champey J, Pavese P, Bouvaist H, et al. Cerebral imaging in infectious endocarditis: A clinical study. Infect Dis (Lond). 2016;48(3):235-40. https://doi.org/10.3109/23744235.2015.1109704
[ Links ]
Novy E, Sonneville R, Mazighi M, el al. Neurological complications of infective endocarditis: new breakthroughs in diagnosis and management. Med Mal Infect. 2013 Dec;43(11-12):443-50. https://doi.org/10.1016/j.medmal.2013.09.010
[ Links ]
Singhal AB, Topcuoglu MA, Buonanno FS. Acute ischemic stroke patterns in infective and nonbacterial thrombotic endocarditis: a diffusion-weighted magnetic resonance imaging study. Stroke. 2002 May;33(5):1267-73. https://doi.org/10.1161/01.str.0000015029.91577.36
[ Links ]
Kim SJ, Lee JY, Kim TH, et al. Imaging of the neurological complications of infective endocarditis. Neuroradiology. 1998 Feb;40(2):109-13. https://doi.org/10.1007/s002340050549
[ Links ]
Hess A, Klein I, Iung B, Lavallée P, et al. Brain MRI findings in neurologically asymptomatic patients with infective endocarditis. AJNR Am J Neuroradiol. 2013 Aug;34(8):1579-84. https://doi.org/10.3174/ajnr.a3582
[ Links ]












 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink