











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkImages in neurology
A 56-year-old, right-handed, previously healthy women, presented with transient global amnesia (TGA), characterized by the sudden onset of anterograde amnesia and confusion with a normal level of consciousness. During the episode, the patient recurrently asked what she was doing and what she had been told, but was able to recognize familiar faces. Mild-to-moderate right fronto-orbital headache was a companion symptom. The episode lasted about 10 hours. No focal deficits were noticed on neurological examination and there was no papilledema. MRI showed a single non-enhancing cystic lesion in the right rostral thalamus, which compressed the foramina of Monroe causing mild dilatation of the anterior horn of the ipsilateral lateral ventricle (Figure, upper panel). Cytochemical analysis of CSF was normal, and stains and cultures for pyogenic bacteria, acid-fast bacilli and fungi were negative. The HIV status was negative. A serum immunoblot for the detection of anti-cysticercal antibodies was negative. Intravenous corticosteroids were given with rapid symptomatic improvement, although she could not remember what happened during the TGA event. (Figure 1)
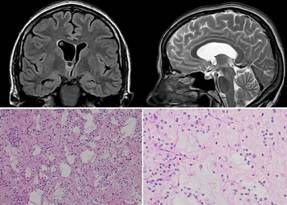
Figure 1 Upper panel: MRI showing a cystic lesion located in the rostral right thalamus and focal hydrocephalus due to enlargement of the anterior horn of the right lateral ventricle. Lower panel: Glio-neuronal tumor of moderate cellularity with microcystic structures and mucoid content (Hematoxilin-eosin 100x) (left), and high-power field (Hematoxilin-eosin 400x) showing floating neurons embedded in the tumor matrix. The tumor cells showed small and round nuclei, and focally clear cytoplasm. Small cystic structures with mucinous content and neurons embedded (floating neurons) were identified. Mitoses, microvascular proliferation and necrosis were not detectable (right).
The patient was referred for surgery. Endoscopic aspiration of the lesion together with fenestration of the septum pellucidum (for relief of focal hydrocephalus) were performed. There were no complications inherent to the procedure and the clinical follow-up after surgery has been uneventfully.
Histopathological examination of the aspirated tissue revealed a glio-neuronal tumor of moderate cellularity with a nodular growth pattern. The tumor cells showed small and round nuclei, and focally clear cytoplasm. Small cystic structures with mucinous content and neurons embedded (floating neurons) were identified (Figure, lower panel). Mitoses, microvascular proliferation and necrosis were not detectable. Cells within the tumor stained for Neu-N and were S-100 and OLIG2 positive. These findings were consistent with the diagnosis of a dysembryoplastic neuroepithelial tumor (DNET), a benign neoplasm that often affects children and young adults(1). This tumor is most often located in the cortex of the temporal lobe. However, rare locations such as the septum pellucidum, the basal ganglia and the posterior fossa have also been reported.
DNET may be asymptomatic or associated with recurrent non-provoked seizures. To the best of our knowledge, this is the first case of a thalamic DNET presenting as TGA, which enhances the clinical spectrum of this benign neoplasm.
TGA is most often related to affection of the temporal lobe and hippocampus. In addition, lesions located out of the temporal lobes but interfering with the Papez circuit have been rarely associated with TGA. Most of these lesions have been of vascular origin (ischemic or hemorrhagic) and have been located in the left thalamus, although occasional reports also pointed to the right thalamus as the site of the responsible lesion (2)(3).

