











 Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
Since the mid-20th century, dynamic changes such as rapid urbanization and growth in production activities have contributed significantly to global economic and human development. However, the methods to achieve this progress have come at a critical cost to the environment [1]. By the early 1970s, human consumption began to exceed the Earth's capacity for regeneration [2]. It became clear that a modern lifestyle, driven by current consumption patterns, is unsustainable, leading to supply insecurity, high levels of waste, climate change, pollution, and global warming [3].
Nevertheless, with the growth of the world population, the contribution of buildings to global energy consumption continues to increase, accounting for over one-third of final energy use and more than 55% of global electricity consumption [4]. The concern with the energy consumption of buildings is worldwide and some contributions to the theme are presented in [5-6]. Specifically in hospitals we have as examples the works [7-8].
Following an increase of approximately 65% in building floor area since 2000, energy demand from buildings has surpassed that of other key sectors, such as industry and transportation [3][9]. In this context, without mandatory and effective policies, it is predicted that approximately 70% of building floor area additions will occur by 2050 [9]. Consequently, enhancing the energy performance of existing buildings through retrofit measures is crucial for the transition to sustainability.
In Brazil, current policies related to building retrofits remain insufficiently robust. According to the Brazilian Energy Research Office (EPE; in Portuguese, 'Empresa de Pesquisa Energética'), one of the key historic initiatives in the building sector is Law 10.295, established in 2001, also known as the Energy Efficiency Law. This law was formulated in response to the so-called blackout crisis that affected approximately 800 Brazilian cities [10]. The Energy Efficiency Law identified buildings as a priority area for promoting energy efficiency mechanisms in Brazil, placing them alongside other products that require energy assessment and regulation. Consequently, the building sector became part of one of the earliest initiatives addressing energy efficiency in Brazil, the National Electricity Conservation Programme (PROCEL; in Portuguese, 'Programa Nacional de Conservação de Energia Elétrica'). The introduction of these policies had a significant impact, with energy efficiency gains of around 21% observed in residential buildings between 2005 and 2018 [10]. However, progress in implementing retrofitting measures remains limited.
Consequently, the building retrofitting process presents both challenges and opportunities [11]. Regarding opportunities, retrofit measures can provide direct benefits, such as reduced heating and cooling costs, as well as indirect benefits [12]. According to the World Green Building Council [13], institutions that adopted a green building approach reported a 23% increase in productivity due to improved glare and brightness control, a 5-14% improvement in test scores in schools with optimal daylight, and a 10-25% improvement in mental function and memory test performance among workers exposed to outdoor views. Furthermore, research indicates that bright sunlight in rooms led to a 22% reduction in the need for pain medication, hospital stays were reduced by 8.5%, and recovery rates were faster in rooms with views of nature [13].
In this context, it is evident that, in addition to improving energy efficiency, building retrofitting can also offer opportunities to enhance human quality of life by reducing exposure to external noise, improving thermal comfort, and enhancing indoor air quality [14]. Therefore, there are significant potential benefits for overall improvements in hospitals and healthcare facilities through retrofitting, which is the primary focus of this paper.
However, despite the numerous advantages of retrofitting, the implementation rate for existing buildings remains low. This low rate is due to several challenges that hinder the retrofitting process, including long payback periods, bureaucratic obstacles, lack of awareness, insufficient data, uncertainties in the decision-making process, and disruptions to ongoing operations [15].
Concerning hospital buildings, additional challenges must be considered. Hospitals house various services and facilities that operate 24/7, including laboratories, nurseries, restaurants, emergency rooms, recovery areas, and surgical suites. Continuous occupancy, the presence of heavy medical equipment, and strict safety regulations further add to the complexity of these buildings [16].
Given the numerous challenges and opportunities, it is evident that, although Brazil has various policies aimed at improving energy efficiency in buildings, none provide specific guidelines for retrofitting hospital buildings. In general, there is no single standard that encompasses energy management regulations tailored to the unique requirements of hospital facilities. Furthermore, due to the lack of knowledge dissemination on this subject and the non-mandatory nature of existing energy efficiency policies for buildings, identifying energy-saving opportunities that account for both technical specifics and financial constraints becomes highly challenging.
Motivated by these factors, this paper proposes a retrofitting methodology for hospital buildings. The methodology is designed to address these challenges by providing a flowchart for selecting the most effective actions for an energy retrofit project. This work aims to clarify which actions should be prioritized within a range of options, considering the constraints imposed by available financial resources.
The structure of the paper is as follows: Section Two reviews related works, outlining the main barriers to retrofitting hospitals and how various countries address this issue. Section Three details the proposed retrofit methodology, including guidelines for selecting the most effective retrofit measures for hospitals based on financial considerations and potential energy savings. Finally, Section Four presents the conclusions and offers suggestions for further research.
LITERATURE REVIEW
According to Papantoniou [17], hospital buildings are often among the least energy-efficient public buildings in many developed countries. Unlike residential and commercial buildings, hospitals operate 24/7, serving thousands of employees, patients, and visitors. Additionally, stringent standards for ventilation, air conditioning, lighting, and thermal comfort significantly increase energy consumption. Shen [18] notes that the energy consumption pattern of hospital buildings exhibits both intermittent and continuous characteristics. As a result, the energy load profile of hospitals varies greatly, leading to substantial energy waste.
Bawaneh [19] indicates that, in U.S. hospitals, the energy intensity is approximately 2.6 times higher than that of other commercial buildings, ranging from 640.7 kWh/m² in the warmest regions to 781.1 kWh/m² in the coldest areas.
This variability highlights how temperature differences across geographical zones significantly impact heating and cooling consumption. In contrast, European hospitals have an average energy intensity of 333.4 kWh/m² [19]. The authors of [17] notes that significant differences in hospital energy consumption patterns arise not only from varying climatic zones but also from factors such as the type of hospital (e.g., general, psychiatric, health center), the condition of the building envelope, insulation levels, energy management practices, and the age and maintenance of mechanical equipment.
There isn´t recent data about electricity consumption in hospital buildings in Brazil. According to Tolmasquim [20], electricity consumption in large hospitals in Brazil is divided as follows: 41% for air conditioning, 26% for lighting, and approximately 5% for water heating. Similarly, Bawaneh [19] reports that in U.S. healthcare systems, major energy consumers include space heating (29%), ventilation (12%), water heating (11%), and cooling (11%). Other research indicates that Heating, Ventilation, and Air Conditioning (HVAC) systems are significant electricity consumers in hospitals worldwide, accounting for 30-65% in India, approximately 51.36% in Thailand, and 44% in the UK [19]. Generally, as noted by Papantoniou [17], the largest electricity consumers in hospitals are cooling machines, air compressors, circulation pumps, HVAC fans, lighting, medical equipment, and office equipment.
In light of this, Buonomano et al. [21] note that hospitals have the highest energy consumption per unit floor area in the building sector, making them prime candidates for cost savings and energy-efficiency measures through refurbishment. Consequently, hospitals can allocate saved funds toward investing in newer technologies to enhance patient care.
Radwan et al. [8] conducted a case study on a hospital in Alexandria, Egypt, with a floor area of 31,019.2 m², focusing on implementing a retrofitting methodology due to the continuous operation of medical devices and air quality requirements in healthcare facilities. The study evaluated energy savings by implementing various retrofitting measures, including reducing lighting intensity, adding wall insulation, and upgrading the ventilation and air conditioning systems. Simulations indicated that adopting a more modern air conditioning system could potentially reduce the hospital's annual energy consumption by approximately 34%. Radwan et al. [8] concludes that the selected retrofitting measures could yield over 41% electricity savings, equivalent to a reduction of 7,068,178 kWh/year. The paper emphasizes that hospitals are distinct from other commercial buildings due to their specific airflow and ventilation requirements.
Buzzi Ferraris [22] examined the Queensland Children’s Hospital in Brisbane, Australia, as part of a Deep Energy Retrofit (DER) project, defined by the IEA EBC Program as a major renovation capable of reducing site energy use intensity by 50%. The study found that replacing fluorescent lighting with LEDs had a payback time of approximately one year. The project also included the installation of photovoltaic windows, which have the potential to save 91 MWh per year with a payback time of 14.2 years. Buzzi Ferraris [22] highlights specific challenges of healthcare facilities, such as high energy consumption due to medical equipment, 24/7 operation, the need for infection and temperature control, and the inclusion of onsite kitchen and laundry services. The study underscores that due to architectural design constraints, not all retrofitting solutions available on the market are optimal. Additionally, Buzzi Ferraris [22] identifies financing as a major barrier in retrofitting projects, as economic benefits are primarily assessed in terms of energy savings, which often makes it challenging for renovation projects to achieve the expected cost-effectiveness.
The authors of [23] studied the implementation of retrofit measures in three different healthcare facilities. In Case Study 1, aimed at reducing energy costs in the Cancer Center and the Emergency Department of a 40-year-old acute-care facility, a new Heating, Ventilation, and Air Conditioning (HVAC) system and LED lamps were installed. Additionally, the building’s electrical supply voltage was upgraded to a 12,000V system. In [23] notes that the scope of energy efficiency measures was limited due to the need to comply with healthcare facility standards for patient care areas. In Case Study 2, the project involved renovating approximately 880 m² of shell space in a hospital’s Radiology department and constructing an Outpatient Clinic. The main criterion for investing in energy-efficient equipment was a maximum payback time of three years. Consequently, the hospital's ventilation system was upgraded to a variable air volume (VAV) system, a heat-recovery wheel system was installed, and the lighting was upgraded. In Case Study 3, the project entailed the construction of a new 52-bed Neonatal Intensive Care Unit on the hospital’s fourth floor. At the time, the hospital's energy cost was approximately 26 dollars per minute.
Hence, the analysis included several retrofitting measures, such as upgrading the lighting system, increasing the outdoor air ventilation rate to a minimum of 30%, sourcing 59% of the total electricity demand from renewable energy, and installing low-flow fixtures for water-use reduction and carbon dioxide sensors to improve outdoor air quality. In [23] emphasizes the importance of ensuring that retrofitting projects for existing hospitals are both energy-efficient and safe for patients. Among the main patient safety concerns during retrofit implementation in the case studies were noise, vibration, dust, and asbestos. However, it is noted that there are currently no standards or guidelines for integrating patient safety with energy efficiency in healthcare retrofit projects. Research conducted in Aguascalientes, Mexico, proposed using Pinch technology to reduce thermal energy consumption in the hospital complex of the Instituto Mexicano del Seguro Social. This study found that the measure could reduce thermal power usage by 38% by adding four heat exchangers to the system, which equates to a savings of 246,000 liters of diesel [17].
In Alonso [24], a comprehensive methodology was proposed to enhance efficiency in multiple chiller plants through targeted data analysis. This study involved data aggregation, filtering, and projection operations to map chillers and the entire electrical plant, enabling the definition and adjustment of operational rules. The chiller plant management software was implemented at the Hospital de León in Spain to determine when to activate or disable a chiller based on various efficiency criteria. This implementation resulted in an electricity savings of 380,000 kWh over the studied year. However, the approach did not guarantee optimal results, and iterative applications of the methodology are required for continued improvement.
Ardente [25] presented significant results from implementing energy efficiency measures in various public buildings. The study included installing solar and wind power plants, upgrading the building envelope, replacing lighting and glazing components, and retrofitting HVAC installations. These measures yielded substantial benefits. Out of an initial energy use of 19,590 GJ/year before the retrofit, an estimated 5,963 GJ/year of energy savings was achieved after the retrofit of these public buildings.
Billanes [26] presents two case studies that explore the influential factors in implementing a 'Bright Green Hospital' and the involvement of stakeholders in this process. In the first case, efficiency actions included the adoption of hospital policies for employees and customers, an energy management program, a natural lighting project for patient rooms, and the replacement of old lighting with LEDs. The second hospital implemented ISO-compliant energy management, set standards for its air conditioning unit, installed LED lighting, and incorporated large windows for natural lighting. Additionally, Pinggoy Medical Center's power management plan features photovoltaic solar panels and a building management system (BMS).
Dainese [27] shared results from an investigation into the energy-saving potential of a polyclinic building within a hospital in the Netherlands. The analysis focused on understanding the building’s characteristics and its energy supply and demand. The findings led to recommendations for energy-saving measures, such as controlled ventilation and lighting rates. These measures aimed to address discrepancies between the number of people present and the building's full capacity, as well as between the designed and installed values of lighting systems. Additionally, the recommendations sought to ensure that the air supply from the ventilation system is adjusted according to occupancy levels rather than remaining constant.
Additionally, Teke [28] presents several energy conservation actions implemented in hospitals across different countries between 2011 and 2020. Portugal was noted for having the most comprehensive actions, addressing various energy systems, including HVAC systems, lighting, and other unspecified systems. The research also details a series of energy efficiency actions and their corresponding reductions in electricity consumption. The actions are as follows:
• Application of advanced and integrated control techniques to regulate HVAC and lighting systems. Potential cost savings rate: 5 to 20% annually.
• Variable Speed Drive (VSD) installation for air conditioning pumps and fans. Potential energy savings rate: 50% (by reducing electric motor speed by 20%, optimizing fan and pump run times).
• Integration of lighting control systems with low-energy lighting. Potential energy savings rate: Up to 30%.
• Implementation of energy efficiency measures for surgery rooms, focusing on reducing the air exchange rate based on occupancy. Potential energy savings rate: Up to 25%.
• Layout changes of cooling equipment for rowless servers in a hospital data center. Potential energy savings rate: 30%.
• Continuous monitoring of energy systems. Potential reduction in annual energy bills: 10 to 15%.
Ludin [29] examined the electricity use of a public hospital in Malaysia, with a total consumption of 11,255,203.45 kWh/year. Proposed energy conservation measures, including awareness campaigns, replacing personal computers with laptops, and updating refrigerators, could potentially reduce total electricity consumption by approximately 429,743.39 kWh/year. This would result in cost savings of RM 152,127.57/year (or $36,510.62/year) and a decrease of 296,522.94 kg/year in CO2 emissions.
A second study focused on electricity load distribution at another public hospital in Selangor, Malaysia, where the annual electricity bill is about RM 8,599,122.56 (or $2,063,789.41). The energy audit recommended additional measures, such as room temperature control, an efficient lighting system, an upgraded Air Conditioning Split Unit (ACSU), and the installation of Variable Speed Drives (VSDs) to regulate motor power. These measures are estimated to incur a total cost of RM 748,606.65 ($179,665.59) with a payback period of 1.78 years. The potential electricity reduction is approximately 1,250,000 kWh/year, resulting in savings of RM 421,706/year ($101,209.44/year) and a reduction of 869 tons of CO2 emissions annually.
It is evident that while the selected case studies demonstrate potential energy savings and health benefits, they also highlight specific challenges associated with retrofitting healthcare facilities. These challenges include obtaining financing, dealing with long payback periods, selecting optimal solutions, ensuring compatibility of new technologies with existing buildings, and addressing a lack of standards and guidelines. Additional issues involve meeting patient safety requirements, complying with healthcare standards, and managing both internal and external coordination.
In this context, Wang et al. [30] developed a comprehensive list of obstacles to energy efficiency within healthcare facilities in China. The study concludes that government actions may have a more significant impact on creating energy-efficient hospital buildings than technical and economic barriers. The main government-related obstacles include a lack of incentives (such as subsidies, rewards, and special funds), the absence of national and industry standards for energy efficiency in healthcare facilities, and the lack of enforceable and mandatory administrative requirements from the government regarding the energy efficiency of healthcare facilities.
PROPOSED RETROFIT STRATEGY
The literature review highlighted several challenges related to retrofitting hospital buildings. In response to these challenges, this section proposes a methodology to guide the selection and implementation of retrofitting measures. The proposed strategy includes:
• A generic process flow diagram outlining the five main stages of a retrofitting project.
• An extensive systematic flowchart that details the process flow, including decision-making steps.
• Two tables categorizing primary and supplementary retrofitting measures.
These schematics form a comprehensive solution that addresses primarily the financial, political, and informational barriers associated with retrofitting hospital buildings. Key differences between retrofit guidelines for general buildings and those for hospitals include the need for specialized training for employees and users, adherence to stricter standards for hospital electrical installations, and ensuring patient safety and privacy, which require compliance with more stringent regulations.
Generic Hospital Building Retrofit Process
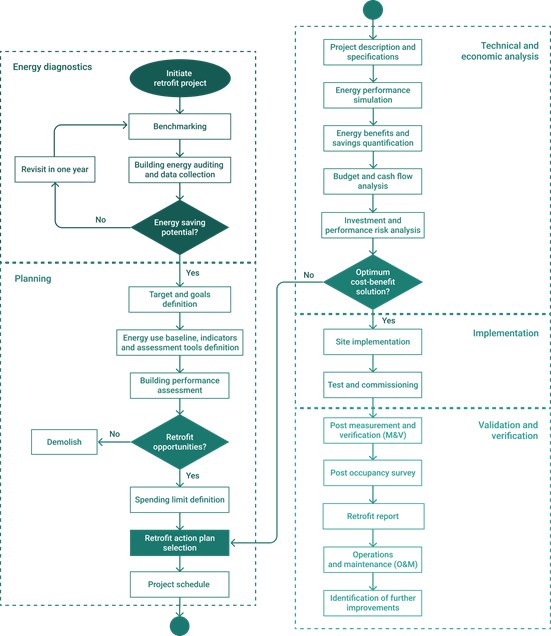
Five main stages have been identified as crucial for overcoming barriers to retrofitting: energy diagnosis, planning, technical and economic analysis, implementation, and validation and verification. These stages are illustrated in the process flow diagram shown in Fig. 1.

Additionally, based on these five key stages, a systematic approach has been developed, as depicted in Fig. 2. This flowchart serves as a decision guide for whether to proceed with or withdraw from the project.
The first stage, energy diagnosis, aims to assess the building’s potential for energy savings. This stage includes benchmarking, conducting energy audits, and preparing a building performance report.
During benchmarking, the goal is to understand how the building’s performance compares to similar structures. This initial step provides baseline information and helps identify opportunities for upgrades.
Energy performance benchmarking provides essential information for formulating energy management plans and identifying opportunities for performance upgrades [31]. According to [32], two indicators are most commonly used internationally for benchmarking in hospitals:
• Annual energy consumption per square meter of the hospital’s building area;
• Annual energy consumption per inpatient bed in the hospital
When adopting these indicators, it's crucial to consider the hospital's specific characteristics and operational aspects. For instance, outsourcing of services such as food and laundry can reduce the hospital's direct energy consumption, resulting in a lower baseline [33].
Therefore, regardless of the project's specific targets, benchmarking is essential for establishing a baseline and identifying the most effective actions. This is the first step towards setting goals and conducting a more detailed analysis of the building through an energy audit.
An energy audit is a fundamental component of any retrofitting project, involving the analysis of energy data and user profiles. It provides a systematic assessment of areas where energy is wasted, how energy is utilized, and where improvements can be made [11]. Given the complexity of hospital facilities, including their use of specialized medical devices and stringent safety requirements, conducting energy audits can be particularly challenging. Therefore, it is advisable to engage a specialist auditor if possible [31].
Finally, after conducting benchmarks and energy audits, an energy performance report must be developed to determine whether the building has energy-saving potential to proceed to the next stage. If the building has no energy-saving potential, the energy diagnosis should be revisited in one year, as depicted in Fig. 2.
Tracking consumption by cost centers through a demand manager is essential to better understand energy systems, define areas of interest, and evaluate opportunities for action without delay. In this regard, both energy losses and usage profiles are necessary variables for evaluating a building’s systems [31]. Generally, some critical questions must be answered to continue an energy efficiency program:
• How much energy is being consumed?
• Who is consuming energy?
• How is energy being consumed, and how efficient are the building systems?
In the second stage, the focus shifts from diagnosing the problem to planning the solution. This stage is referred to as the planning stage. In this step, both qualitative goals and quantitative targets must be defined. According to [31], many hospitals establish both short- and long-term goals. By setting short-term goals, immediate cost savings can accumulate over time, which may help fund longer-term upgrades. Defining these goals is also beneficial when assessing energy audit data.
At this stage, a more in-depth assessment and diagnosis of the building’s performance are considered decisive factors. Here, performance assessment is crucial for evaluating the life cycle environmental and economic factors that will determine whether it is better to retrofit the building or demolish and rebuild it, as depicted in Fig. 2. Since retrofit options typically have lower life-cycle economic costs than rebuilding, the latter option might be considered only in critical situations [34].
Once the decision is made to proceed with the retrofit, it is important to establish a well-defined scope to ensure the project plan is functional. This step includes defining the baseline, indicators, and assessment tools to be evaluated during and after the retrofit. Additionally, it involves selecting the retrofit level, which can be categorized as economical, standard, or sophisticated.
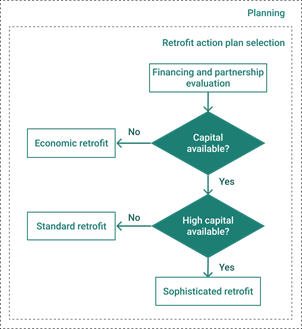
In this regard, the flowchart presented in Fig. 3 illustrates the "Retrofit Action Plan Selection" step within the planning stage. Specifically, the "Selection of Retrofit Actions" sub-flowchart is part of the "Project Schedule," a crucial phase in the proposed methodology flowchart. This excerpt aims to guide the selection of a retrofit plan that aligns with financial constraints. To select a feasible plan, it is essential to define the project’s spending limits, taking into account available financing and partnership options. Establishing the retrofit level based on financial considerations helps narrow down the possible retrofit measures, making the decision process more straightforward.
In low-budget scenarios, the project is typically limited to an economical retrofit, which may include only operation and maintenance measures (O&M) or minimal emergency actions. If the budget permits more than just O&M actions, the project may reach a standard level, incorporating more advanced measures. In cases where there are numerous retrofit opportunities and substantial capital available, a sophisticated retrofit project may be considered, potentially including measures such as installing photovoltaic systems and cogeneration technologies.
The planning stage concludes with the selection of retrofit measures and the development of a project schedule. This timetable outlines the deadlines and milestones that must be met to ensure timely project completion. Given that the project schedule is dependent on the chosen retrofit measures, a detailed and comprehensive guide is essential for making these decisions, as elaborated in the following section.
It is important to note that the complexity of retrofitting actions extends beyond their selection. Implementing these actions presents additional challenges, particularly for hospitals and other healthcare facilities. Many of these challenges can be anticipated during the planning stage. Healthcare buildings have unique characteristics, such as continuous operation, patient security requirements, and stringent sterilization and cleaning protocols [35].
To ensure the well-being of patients and staff, retrofitting hospitals must minimize impacts on their daily operations and maintain the constant functionality of critical hospital systems. It is crucial to evaluate equipment usage in building controls beforehand. According to [36], hospitals need careful zoning to provide isolation and create negatively pressurized spaces to minimize the risk of infection transmission. Therefore, the retrofit project must account for scheduling measures such as dust control, patient relocation, and the use of negatively pressurized anterooms. Additionally, coordinating the retrofit schedule with the nursing and hospital management teams is essential to align the hospital's operations with the retrofit implementation.
Additionally, it is crucial to ensure that anyone working on-site during the retrofitting project, especially in inpatient rooms or other sensitive areas, is healthy and meets all medical requirements for working in such environments. Therefore, careful planning must include reviewing hospital codes, verifying health and safety regulations, and scheduling interruptions to hospital operations to facilitate the implementation of retrofitting measures [35].
The third stage involves the technical and economic analysis of the selected retrofit plan. During this phase, various analyses and studies are conducted to prepare for the implementation of the chosen measures. This includes performing energy performance simulations, quantifying potential energy savings, detailing the project description and specifications, examining budget expenditures and cash flow, and assessing performance and investment risks.
In this regard, the economic and risk analyses are crucial for deciding whether to proceed with the retrofit project or withdraw. Economically, several methods can assess the feasibility of each retrofit measure, including net present value (NPV), internal rate of return (IRR), benefit-cost ratio (BCR), and payback time. Risk analysis is equally important, as hospital retrofitting involves numerous uncertainties. This analysis provides decision-makers with the confidence needed to select and implement the most appropriate retrofit solutions. Key uncertainties include the estimation of savings, energy use measurements, weather forecasts, changes in consumption patterns, and system performance degradation. These factors must be evaluated to ensure that the chosen solution is the most viable option. Thus, to proceed to the implementation stage, the analysis must demonstrate the best cost-benefit alternative.
The fourth stage involves the on-site implementation of the selected retrofit measures. During this phase, testing and commissioning are conducted to ensure that the building achieves optimal energy efficiency. Following the implementation and adjustment of retrofit measures, measurement and verification (M&V) methods must be employed to monitor the performance of the energy systems [37]. This stage also includes a post-occupation survey to assess occupant and owner satisfaction with the retrofit's overall results. Additionally, the outcomes of the retrofit and the operation and maintenance (O&M) methods are documented in a report. This report should detail the building’s efficiency parameters and evaluate potential areas for further improvement.
Retrofit Measures for Hospital Buildings
Assuming that each main efficiency action affects subsequent actions, this section emphasizes the importance of following a systematic criterion when selecting retrofitting measures for a building. According to [31], the staged upgrade approach seeks to enhance building systems by adhering to a specific order, where improvements in one system influence others. For instance, upgrading lighting systems first can alter the thermal load, which in turn impacts the design of the cooling systems. Similarly, a reduction in energy consumption due to improved lighting can also affect the performance and sizing of the building’s photovoltaic system.
In light of this, the paper proposes a methodology for selecting the appropriate retrofit plan. Two distinct tables of important retrofitting measures have been developed to differentiate between actions that directly reduce energy consumption (primary measures) and those that rely on the building’s consumption history (supplementary measures). Each table prioritizes the actions to ensure that each upgrade measure considers how changes will impact subsequent actions.
The rationale for distinguishing between these two lists is to prevent over-dimensioning of power generation systems, avoid unnecessary investments, and prioritize immediate actions that reduce electricity costs. As financial factors are a significant barrier in retrofitting projects [30], the methodology aims to minimize related expenses by avoiding unconstrained actions. By adhering to the defined priorities, it is anticipated that the building will achieve maximum energy savings.
The retrofitting actions illustrated in the primary and supplementary measures include auxiliary loads, lighting, HVAC systems, flow pumping systems, water heating, power generation systems, data analysis of electricity bills, and power quality. The criterion for selecting these actions involved a technical analysis of the appliances and components, along with an evaluation of the most energy-efficient systems available on the market. This approach aims to simplify the O&M stage by leveraging predictive, preventive, and corrective maintenance activities [31].
The following subsections will illustrate the impact of these measures. It is important to note that technological advancements over recent decades have led to diverse options for reducing electricity consumption and retrofitting measures. For instance, replacing incandescent luminaires with LED lamps can now include advanced features such as presence detection systems [36].
Additionally, as identified during the literature review, one of the factors that complicate the success of retrofitting projects is the difficulty in decision-making and the inadequate selection of retrofit actions [30]. As discussed in Section 3, determining a retrofit level based on economic aspects helps narrow down the possible retrofit actions. However, in addition to financial considerations, the selection of retrofit measures should also account for technical aspects [21]. In this context, the flowchart presented in Fig. 4 illustrates the process for prioritizing and selecting primary and supplementary measures during the project schedule
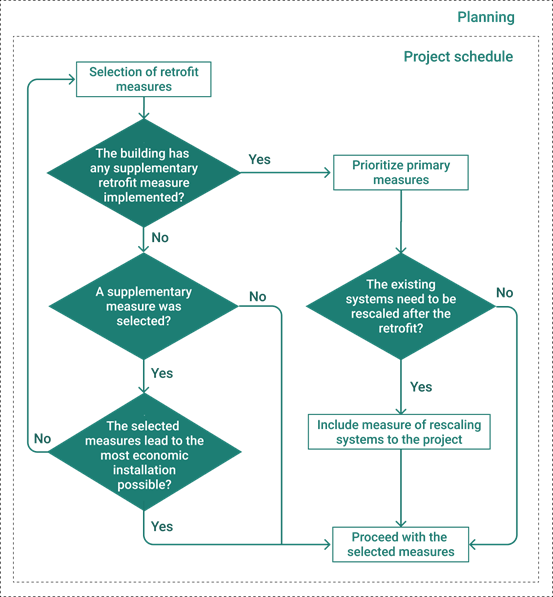
The process begins with a broad selection of retrofitting measures based on economic considerations. It then progresses through a pipeline that refines the options according to the building’s characteristics. Initially, it is assessed whether the building has already implemented any supplementary actions, such as photovoltaic generation. If so, primary retrofit actions should be prioritized to ensure optimal performance of the building systems. This reduction in consumption might necessitate rescaling systems before proceeding with the selected measures.
Conversely, if the building has not yet implemented any supplementary measures, it is essential to determine whether such measures are needed. If so, primary actions must be implemented first. Subsequently, when technically and economically analyzing the supplementary measures, it is crucial to consider that the primary measures will have been completed beforehand.
Primary Retrofit Measures
From sources such as [31], [32], and [36], it is evident that numerous efficiency measures can be implemented in a hospital retrofitting project. Consequently, this preliminary work has selected the most relevant measures for hospital energy systems, encompassing both end-use and generation profiles. Fig. 5 presents various individual retrofitting measures specifically aimed at reducing energy consumption in hospitals.

Some of these measures may impact multiple energy systems within a hospital. Thus, the developed table facilitates visualization of the potential for simultaneous implementation of several immediate retrofitting measures.
These measures are directly related to the implementation of energy-efficient technologies. It is important to recognize that energy efficiency aims to delay the need for new energy developments by preserving the environment and altering the electricity consumption patterns of individuals and institutions. Additionally, it seeks to advance technology, introduce energy-efficient appliances to the market, and promote rational energy use. In this context, careful project planning is crucial to achieving successful energy efficiency and ensuring lasting results.
It is prudent to reduce the loads of medical and office equipment, as well as laundry and kitchen appliances, before making HVAC systems more efficient or implementing other advanced measures. A straightforward approach to reducing these loads is to replace such devices with high-efficiency equivalents. This illustrates how adhering to a prioritized order for implementing retrofitting actions can significantly contribute to the project's success.
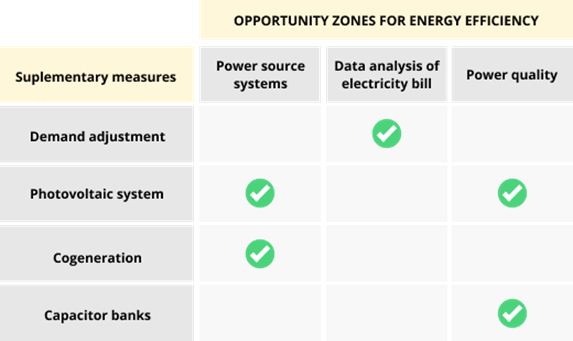
Supplementary Retrofit Measures
After implementing the efficiency measures that minimize energy waste the most, you can proceed with retrofitting actions that depend critically on the building’s electricity consumption history. Fig. 6 summarizes some of these measures.
Similar to Fig. 5, Fig. 6 relates efficiency measures specified on the vertical axis with the opportunity zones for energy efficiency, set on the horizontal axis, that are impacted by these measures.
CONCLUSIONS
This paper addresses the critical issue of energy efficiency in hospital facilities and presents a systematic methodology for retrofitting hospital buildings. Based on the development of the proposed methodology and the literature review, the following findings are highlighted:
1. Retrofitting Existing Buildings: It is essential for advancing sustainability and achieving long-term energy savings.
2. Energy Efficiency in Hospitals: Hospitals are among the least energy-efficient buildings, thus offering significant potential for energy savings.
3. Specialized Technical Team: Effective coordination of an Energy Saving Plan within a hospital requires the formation of a specialized technical team.
4. Training and Support: It is crucial to prepare and provide teams to train employees and users on maintaining and enhancing the results achieved through energy efficiency measures.
5. Job Creation: Investments in energy efficiency can drive job creation, particularly when high energy efficiency potentials are identified.
6. Challenges in Implementation: Despite its advantages, retrofitting implementation remains low due to economic, political, and informational barriers. Hospitals face additional challenges, including continuous occupancy, complex medical equipment, and patient safety requirements.
7. Strengthening Policies: There is a clear need to reinforce energy efficiency (EE) policies for buildings to make them compulsory.
8. Decisive Moments: Three critical stages before implementing a retrofit project include energy diagnosis, planning, and performance and risk analysis.
9. Uncertainty and Methodology: Due to the high level of uncertainty associated with building retrofitting investments, developing methodologies that facilitate more straightforward decision-making is essential.
These findings were crucial in developing a comprehensive strategy to make hospital retrofitting feasible. The methodology primarily addresses financial, political, and informational barriers. Key goals include simplifying the decision-making process and reducing retrofitting expenses by avoiding unconstrained actions. To achieve these objectives, the methodology proposes classifying measures into primary and supplementary categories and adopting a staged retrofit strategy.
By systematically evaluating each obstacle, the approach aims to streamline the retrofitting process, ensuring that actions are both cost-effective and impactful. The classification helps prioritize immediate measures that directly reduce energy consumption, while the staged strategy ensures a logical progression of retrofitting actions based on their impact and feasibility.
Considering that each upgrade measure affects subsequent retrofitting actions, the proposed strategy distinguishes between two types of retrofit measures: primary and supplementary. This approach helps prevent over-dimensioning of energy generation systems, avoids unnecessary investments, and prioritizes immediate actions to reduce electricity costs.
In conclusion, this paper initiates an important discussion on retrofitting hospital buildings and highlights study and policy gaps that impede such projects. For future research, it is recommended to conduct extensive studies on operational issues in hospital retrofitting and to perform regional analyses of current retrofitting codes.

